Women are not small men – we need to learn how to harness our power. Thanks to pioneering women such as Dr Stacy Sims, this area of science is gaining more mainstream focus. When it comes to sports nutrition and a training plan, women are typically treated the same as men. Women are not frequently studied in a research context as our cycle makes it inconvenient with too many ‘confounders’ to be able accurately report results. So, on the whole (there are exceptions) we get told to do the same as men despite clear physiological differences.
Did you know your period can be an ergogenic aid? The female hormone cycle is one of the most obvious areas in which we differ from men in terms of physiology. By understanding your cycle, the different role each hormone plays and when it is dominant, you can learn to understand your body and how to manipulate your training and your diet to suit where you are in it and access your full potential.
So a quick recap on a typical female cycle:
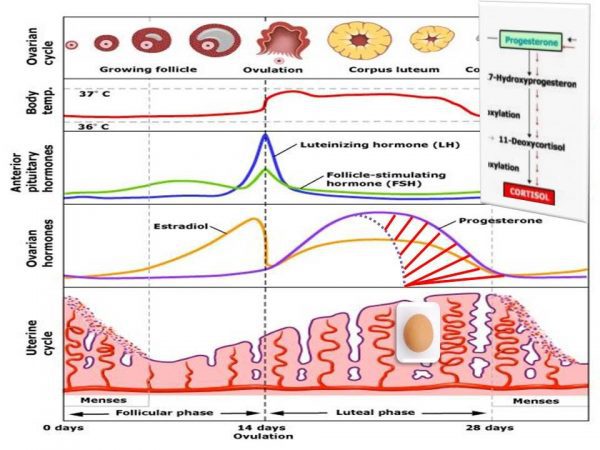
- A menstruating woman’s cycle can be split principally into two halves – the first is the follicular phase (or proliferative phase) and the second in the luteal phase (or secretory phase). The dividing line between the two is determined by when a woman ovulates.
- The first day of a cycle is counted from the first day of your bleed and ovulation typically occurs 10-14 days after this. A typical cycle can vary in total number of days from 21 to 35.
- Oestrogen rises during the first phase, takes a dip when an egg is released during ovulation, and then rises again before dipping off before the menses. Progesterone rises in the second half of the cycle preparing the body for implantation – if this does not occur both progesterone and oestrogen drop off and bleeding occurs.
- As both progesterone and oestrogen peak in the second half about 4-5 days before your period, is a typical time for PMS symptoms to be felt. This second half when both hormones are high is also known the ‘high hormone’ phase.
- Without sufficient luteinising hormone, ovulation will not occur. Without ovulation, progesterone will not be stimulated and a ‘flat’ cycle with occur. You can read more about this here
Some of oestrogen’s physiological functions and it’s impact on athletic performance:
- Oestrogen leads to fat deposition – which is why curves occur when puberty hits. Higher oestrogen also results in relying less on carbohydrates as a fuel source for general metabolism, using more fat instead – this can make us good fat burners and great at endurance sports. However, when oestrogen is at its highest just before ovulation and just before menses, this means we tend to hang on to stored glycogen (the link also with weight gain and water retention) and it can be harder to reach those higher intensities without taking on extra glucose fuel sources. When training in the anaerobic zone, glucose is needed and fat simply doesn’t ‘cut it’ (1). Ensuring you have extra carbs at these points in your cycle not only will help you reach your set targets but also helps prevent your body utilising muscle as a source of fuel.
- Oestrogen can result in decreased stiffness in tendons and ligaments making women more prone to injury when it is high (2) Ensuring adequate nutrient status for collagen (type 1) production- this includes vitamin C for cross-linking of proteins – is important as well as listening to your body and taking potentially longer recovery periods between harder sessions if you feel any niggles.
- How women respond and feeling during ovulation and when oestrogen peaks in the first half is very individual – some women can feel a bit ‘flat’ and others are ‘on fire’. If you track you may know which are you. If you are someone who feels really good at this point, go for it, push hard and get the training adaptations in.
Some of progesterone’s physiological functions and it’s impact on athletic performance:
- Progesterone is catabolic and increases muscle breakdown. Thus, during the high hormone phase (second half) and particularly towards the peak, repair of tissue from breakdown during training maybe slower. Timing of protein at this point becomes more important as well as ensuing sufficient quantity – a focus on sources of branch chain amino acid may also be helpful (leucine, isoleucine and valine). The right amount of (quality) protein and the right time will not only help offset the catabolic impact of progesterone but reduces signalling to the body to store fat which can occur when oestrogen is high.
- Progesterone competes for the same receptors as a hormone called aldosterone that is involved in regulating blood (plasma) volume. So when progesterone is high, blood volume can be lower which can lead to lower blood pressure and cardiac output. By increasing your fluid intake with electrolytes may help offset this.
As a woman, we often may worry about getting period just before a big race or training day but in fact, once your period starts, your hormones can be in your favour. Hormones start to drop off and the body moves out of preparing for pregnancy mode and ready to re-divert resources elsewhere such as muscles and even to your brain so perceived effort may be lower. Even if your race does fall when your hormones are at their highest, it has been shown that VO2 max and lactate threshold don’t change during the month, although perceived effort may be higher. If you suffer from cramping, additional magnesium and omega-3’s to offset the rise in prostaglandins in the run up to this point (5-7 days) may help.
What else is going on? Body temperature of a woman rises in the second half of her cycle – depending on your race conditions, this may either work with you or against you. In general women sweat less – you’ve probably sat next to that guy in the spin class who looks like’s he’s been swimming while you have barely a sheen to your skin. However, progesterone can result in a greater sweat rate and loss of sodium. Additional salt intake during the second half, particular during and post longer training sessions, can be beneficial.
What about women who are on the contraceptive pill so you don’t bleed or where your cycle is irregular? It is important to understand that a contraception induced bleed is not a real bleed so the above rise and fall of hormones will not necessarily apply to you. Contraceptives work to suppress ovulation. So whilst there may be a convenience to not having a period, you are arguably missing out on some significant potential training adaptations if you knew how to use your cycle to your advantage. For athletes that travel, be aware that certain contraceptives can increase the risk of DVT’s via increased risk of blood clotting (3), (4). There are other potential disadvantages to do with signalling from the brain (HPA axis) and feedback loops with other hormones but that I will save for another day.
For women with irregular cycles or missed periods, perhaps diagnosed with PCOS, endometriosis, fibroids or ‘simply’ irregular cycles, I recommend you get some help to understand what may be going here. Often there is an underling source of inflammation that needs to be addressed or it may be you are under-fuelling, not eating enough carbohydrates for your requirements. Relative Energy Deficit Syndrome (REDS), defined as a pattern of disordered eating, amenorrhoea and decreased bone density, can have a long term impact on the body far beyond missing a few periods so please do seek help or advise if this applies to you. Disordered eating and eating disorders (not the same) have risen significantly through lock-down and athletes are a vulnerable population.
Last but not least, what about peri-menopause and menopause? During peri-menopause time, large fluctuations of oestrogen (surges) are common which is hypothesised as one of the reasons women experience hot flushes as oestrogen is known to influence the temperature regulating area in the brain, effectively creating a thermostat where the on-off button is being flicked each time you get a surge and drop. Another job of oestrogen’s is to sensitise cells to both serotonin, our happy hormone, and insulin resulting in reduced ability to metabolise sugar. What can you do? An overall dietary and nutrient assessment here may be required as the impact of altered glucose metabolism can spread beyond the training window. Assessing your overall carbohydrate intake and in what form they come is important, understanding the link with cortisol and ‘stress’, the importance of supporting your adrenal glands that are required to take over some of the production of oestrogen as ovary function declines are all going to be part of this. However, please don’t just accept this changes as part of ageing! Of course we all age and our body will change too but understanding our physiology allows us to adapt and minimise the impact.
Katherine is a degree qualified Nutritional Therapist, mother of two and a GB Age Group triathlete with additional training in eating disorders. If you want to find out more about how Katherine can help you please contact her here.